 What criteria do we use to determine the safest, most efficient and most effective way to perform endodontics given our present state of technological skills? Do we want to make a minimal preparation that sacrifices as little dentin as possible assuming the tooth will retain more of its preoperative strength? Doesn’t that leave open the possibility that we will not cleanse the canal as well leaving tissue and bacteria as continuing sources of breakdown? On the other hand, won’t greater tapered preparations cleanse the canal more thoroughly preparing a space that can be irrigated more effectively? While this is true, greater tapered rotary preparations, continuous and interrupted, have been documented in multiple research studies to induce micro-cracks, reduce the resistance to vertical fracture and increase the amount of leakage after obturation. It seems that the consequences of either minimal or more aggressive instrumentation have their drawbacks. Yet, both approaches are for the most part producing round holes with the distinguishing differences being the diameter of the apical preparation and the taper along length.
What criteria do we use to determine the safest, most efficient and most effective way to perform endodontics given our present state of technological skills? Do we want to make a minimal preparation that sacrifices as little dentin as possible assuming the tooth will retain more of its preoperative strength? Doesn’t that leave open the possibility that we will not cleanse the canal as well leaving tissue and bacteria as continuing sources of breakdown? On the other hand, won’t greater tapered preparations cleanse the canal more thoroughly preparing a space that can be irrigated more effectively? While this is true, greater tapered rotary preparations, continuous and interrupted, have been documented in multiple research studies to induce micro-cracks, reduce the resistance to vertical fracture and increase the amount of leakage after obturation. It seems that the consequences of either minimal or more aggressive instrumentation have their drawbacks. Yet, both approaches are for the most part producing round holes with the distinguishing differences being the diameter of the apical preparation and the taper along length.
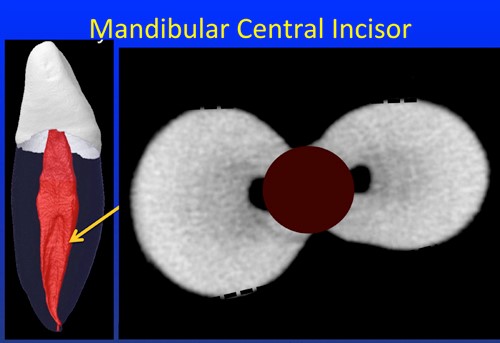
An interesting feature of pulpal anatomy is the variety of shapes it may have. Conical anatomy is pretty much limited to maxillary centrals and laterals. Canines generally have a pulp several times wider in the bucco-lingual plane than the mesio-distal. Premolars most often have highly oval anatomy in the bucco-lingual plane further complicated by the presence of concavities on their mesial and distal axial walls. Maxillary molars generally have 3 or 4 canals with the mesio-buccal canal often being tear drop in shape with the longer diameter in the bucco-lingual plane. The palatal root is the only root in the mouth that is most often wider in the mesio-distal plane than the bucco-lingual. The mesial canals of mandibular molars generally wider in the bucco-lingual plane are often connected by a thin isthmus of pulpal tissue. The distal root can be anywhere from 2 thin canals, round in cross-section to a single canal wide in the bucco-lingual plane and quite thin in the mesio-distal plane. The mesial and buccal roots of molars have the added complexity of being highly concave on their furcal surfaces.
Knowing what we do about pulpal anatomy and the roots within which they reside, is there a strong correlation between the anatomy as it is and the shapes we impose on those canals in the process of cleansing, shaping and obturating them? I believe for the most part the answer is obvious and must be answered in the negative. Why do I say that? Let’s examine what we are using to shape canals. While techniques vary in detail, generally we are attempting to negotiate to the apex of the root to establish the initial glide path. For that task, K-files are generally employed using a watch winding motion combined with a push/pull stroke. The clockwise portion of the watch-winding stroke engages dentin and the pull stroke shaves dentin away from the canal walls as the predominantly horizontal flute construction of the file is now more or less at right angles to the plane of motion. These same horizontally oriented flutes tend to impact debris and any pulp tissue apical to the instrument’s tip as the down stroke is employed in negotiating more deeply. Knowing this to be a problem, lateral shaping would only exacerbate debris impaction resulting in an increased incidence of loss of length. By staying centered within the canal less debris is generated and the chances of apical impaction are reduced.
Yet, from the earliest K-files used, the technique imposes the need for staying centered, eliminating the ability to remove tissue from what will often be the presence of buccal and lingual extensions. We should be very clear that the need for tissue removal in the extensions persists. The fact that the K-files are poorly designed to get there does not negate the need. With the introduction of rotary NiTi, continuous and interrupted, the initial K-file shaping became known as the glide path, preparing the canal to a minimum of a 20/02 in most cases.
Rotary NiTi was introduced as a paradigm improvement over the use of K-files alone or in conjunction with peeos and gates gladdens based on its increased flexibility compared to stainless steel allowing it to be used in tapers much greater than the 02 stainless steel is limited to. Greater tapers gave the instrument the property of being very flexible in its apical portion where it is most likely to incur curved canals and more robust where it is required to gain straight line access in the coronal portion of the canal. A good deal of the hand fatigue associated with the manual use of K-files was eliminated because the rotary NiTi instruments are engine-driven.
The Achilles heel of rotary NiTi is its need to be used in a crown down fashion a technique that demands the removal of excess amounts of dentin in the mesio-distal plane. While this is no problem for maxillary centrals and incisors that have conically shaped pulpal anatomy to begin with, it presents a problem for just about every other tooth in the mouth. Dentists may not necessarily see the problems with over preparation in the mesio-distal plane. Many have been taught to see the greater tapered shaping of canals as a step forward over the more raggedy preparations produced by K-files alone. Yet, one only needs to look at the mesio-distal dimensions of molar pulp tissue to see it is at its largest quite thin and almost parallel in the mesio-distal plane. What we see after rotary preparations is often a mesio-distal preparation that is several times wider than the original pulpal width and a taper that far exceeds what existed previously.
Research documented over the past 8 years is now correlating this form of shaping generated by a rotating engine as responsible for producing dentinal micro-cracks and reducing the resistance to vertical fracture. Furthermore, similar to the K-files inability to work the buccal and lingual extensions of highly oval isthmus like canals, the rotary NiTi instruments even more are limited to staying centered lest they have a greater tendency to separate. Where K-files are guilty of leaving tissue in the buccal and lingual extensions, rotary NiTi is guilty of the same while at the same time removing excessive tooth structure in the mesio-distal plane.
The manufacturers have taken notice of the conflict inherent in the present way their systems are doing things. Today, they are offering 02 tapered rotary NiTi instruments to replace K-files after negotiating them to a 10 and reducing the tapers of their final canal preparations. These instruments are designed as reamers with predominantly vertically oriented flutes that will shave dentin away as they rotate clockwise. The manufacturers are now responding to the detrimental impact of greater tapers and the inefficiencies of K-files. They continue to employ full rotations, continuous and interrupted to drive the instruments ignoring the clearly established relationship between rotation around a curve and the production of micro-cracks as well as the stresses generated in the instruments that can lead to separation, a factor that until completely resolved will discourage dentists from using them with vigor against the buccal and lingual extensions of oval canals.
From my perspective it is obvious that the use of K-files, greater tapered instruments and rotation have caused more problems than they have solved. I would replace K-files entirely with 02 tapered stainless steel reamers unrelieved through a 10 and relieved with a flat along their entire working length starting with a 15. These instruments will negotiate to the apex with far less resistance and minimum potential to impact debris apically. The vast majority of the cleansing and shaping would be done with 02 tapers with an 04 tapered shape being the maximum in most cases. The instruments (except for the first determining the length) are powered mostly by a 40-45º reciprocating handpiece oscillating at 3000-4000 cycles per minute. With such a short arc of motion, the instruments are virtually immune to breakage finally giving the dentist the confidence to use them vigorously against the buccal and lingual extensions from the 06 tipped stainless steel reamer onwards. It should be noted that once an instrument can be worked against all the canal walls, the final shape will be larger than the instrument, at least in the wider plane. It is the fact that the instruments now have the potential to extend their cleansing and shaping into these recessed areas with complete safety to both the instruments and the roots that separates this approach from all the others.
Regards, Barry